TRT Optimization & Side Effects Troubleshooting Guide
This document combines best practices for testosterone dose titration and a detailed troubleshooting guide for common TRT-related side effects. It is designed for both patients and clinicians to support long-term optimization of testosterone replacement therapy while minimizing side effects and maximizing benefits.
🟩 Comprehensive TRT Dose Titration Strategy
🔹 Why Dose Titration Matters
Testosterone optimization therapy (TOT) is not simply about replacing low levels with a static dose. Instead, it is about methodically increasing testosterone levels in a way that:
Respects the body’s adaptation timeline
Reduces risk of overshooting or side effects
Allows stable neurological, metabolic, and hormonal changes
Too many practitioners or patients jump to higher doses too quickly. This can result in side effects like sleep disruption, emotional dysregulation, elevated hematocrit, or cardiovascular strain. The goal is to titrate slowly and strategically.
🔹 Common TRT Preparations & Delivery Considerations
Testosterone cypionate/enanthate (injectable)
AU/UK/EU: 250 mg/mL
US: 200 mg/mL
Insulin syringes (0.5 mL) are commonly used
Each tick = 5 mg (if 250 mg/mL) or 4 mg (if 200 mg/mL)
Example: 0.1 mL on a 250 mg/mL syringe = 25 mg
Doses should only be adjusted in exact measurable units — this avoids inconsistent administration and incorrect increases.
🔹 Initial Dosing Strategy
Most patients will begin TRT on a conservative dose based on the delivery concentration:
0.2 mL 3x/week (250 mg/mL) = 150 mg/week
0.2 mL 3x/week (200 mg/mL) = 120 mg/week
While these doses may not be “optimal” yet, they are safe and stable starting points.
Important:
The body requires weeks to months to adjust to new androgen levels.
Each step up increases androgen receptor activity, affects neurological pathways, and influences other hormonal systems (e.g., estrogen, DHT).
🔹 Titration Progression Timeline
Assuming stable labs and tolerable symptoms:
Step | Weekly Dose (250 mg/mL) | Per Injection (3x/week) | Notes |
|---|---|---|---|
1 | 150 mg | 0.2 mL | Starting dose |
2 | 165 mg | 0.22 mL | After 3–6 months |
3 | 180 mg | 0.24 mL | If still symptom relief needed |
4 | 195 mg | 0.26 mL | At 6–12 month mark |
5 | 210 mg | 0.28 mL | Only if no side effects |
6 | 225 mg | 0.30 mL | Max for most cases |
Note: These adjustments are based on biological feedback, not subjective impatience. Every dose change should be accompanied by a symptom log and blood test.
🔹 Dosing Frequency Recommendations
Daily injections (best stability) – Ideal for sensitive individuals or peak optimization
3x/week (optimal balance) – Most common and effective approach
2x/week (minimum acceptable) – For those with low compliance or limited flexibility
🔹 What You Should Be Tracking:
Energy, libido, mood, cognition
Sleep quality and temperature regulation
Hematocrit, blood pressure, lipid panel
Total T, Free T, SHBG, Estradiol (E2), DHT
🔹 Objective of Optimization:
The goal is to reach a personalized sweet spot, often defined by:
Free T in upper-normal or slightly supraphysiological range (e.g., 1000–1500 pmol/L)
No negative biomarkers (hematocrit, BP, liver enzymes)
Minimal or no side effects
Subjective well-being, stable libido, cognition, recovery
With that foundation, we can now explore how to manage common TRT side effects.
🟥 TRT Side Effects Troubleshooting Guide
1.
Acne
Timing: During titration or early phase.
Causes: Hormonal fluctuations, excess oil, poor skincare, diet, inflammation.
Fix: Improve hygiene, review diet, add zinc or topical treatments. Usually resolves in 2–3 months.
2.
Sleep Disruption / Insomnia
Timing: After a dose increase.
Causes: Overstimulation, high cortisol.
Fix: Cut caffeine, optimize sleep hygiene, lower dose if needed, try magnesium or glycine.
3.
Night Sweats / Excess Sweating
Timing: High dose or during titration.
Causes: High DHT/E2, CNS activation.
Fix: Check estradiol/DHT, lower dose, improve bedroom cooling, evaluate sympathetic tone.
4.
Mood Swings / Irritability
Timing: Rapid changes in protocol.
Causes: Hormone shift, emotional dysregulation.
Fix: Slow titration, stable dosing, stress management, therapy.
5.
Facial Flushing / Redness
Timing: Post-injection or peak serum.
Causes: Vasodilation, high BP.
Fix: Track BP, lower peaks by increasing injection frequency.
6.
Elevated Hematocrit / Hemoglobin
Timing: 3–6 months into TRT.
Causes: Increased erythropoiesis.
Fix: Donate blood if >53%, hydrate, reduce dose.
7.
Lipid Changes (↑ LDL, ↓ HDL)
Timing: Weeks to months after TRT starts.
Causes: Dose-dependent, individual variability.
Fix: Healthy fats, cardio, reduce dose, add omega-3s.
8.
High Liver Enzymes (ALT/AST)
Timing: Sporadic or after hard training.
Causes: Exercise-induced or liver stress.
Fix: Rest 2–3 days before labs, recheck if ALT >60.
9.
Water Retention / Puffiness
Timing: Early TRT or dose bump.
Causes: Elevated estrogen, sodium.
Fix: Lower salt/carbs, hydrate more, check E2.
10.
Low Libido Despite TRT
Timing: Ongoing or post-stabilization.
Causes: DHT/Prolactin issues, lifestyle, mental health.
Fix: Check prolactin/DHT, reduce alcohol/stress, address psychological factors.
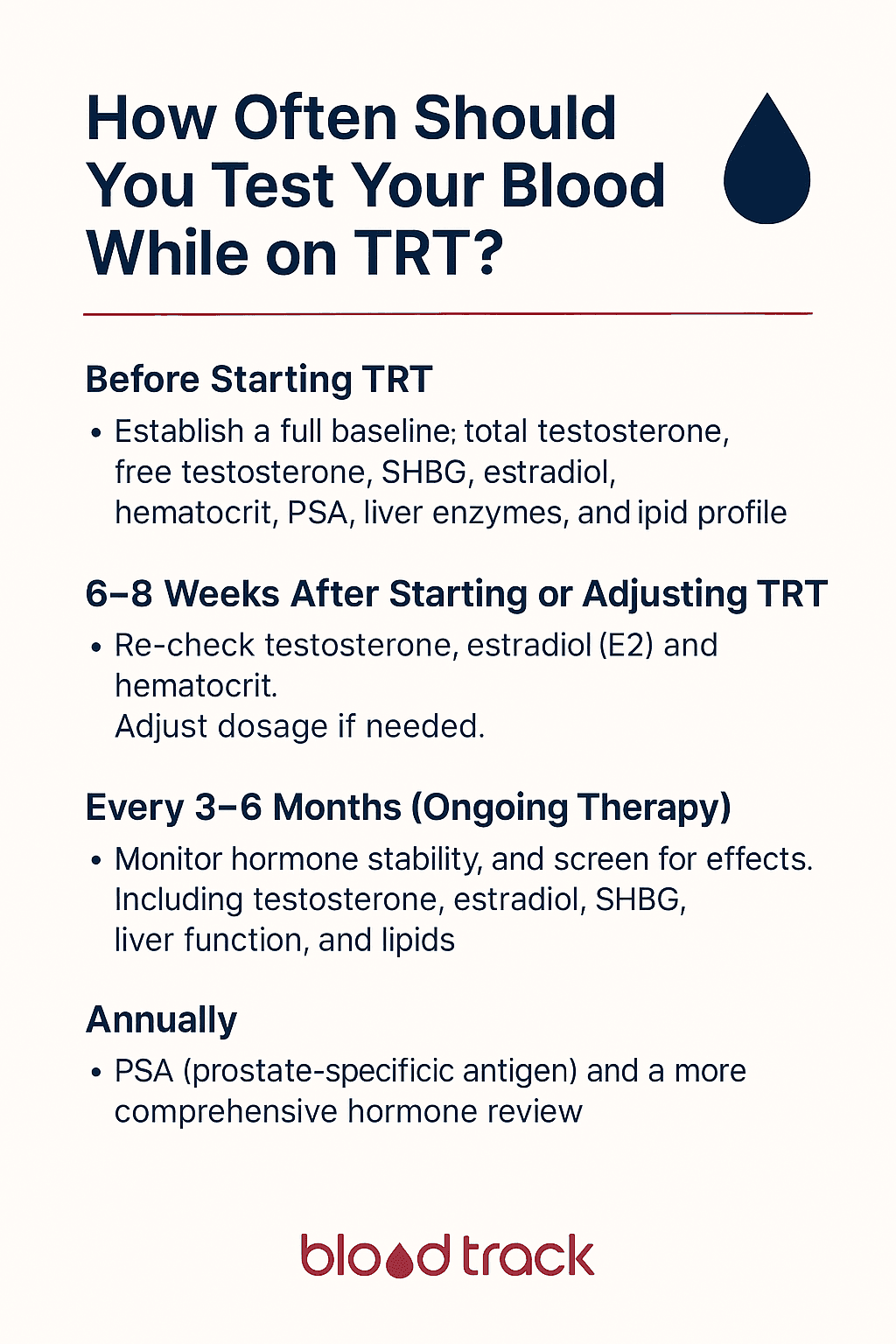
🔎 Diagnostic & Tracking Recommendations
Track Labs & Symptoms:
Total Testosterone
Free Testosterone
SHBG
Estradiol (sensitive E2)
DHT
Hematocrit / Hemoglobin
Lipids (LDL, HDL, Triglycerides)
ALT/AST
Prolactin
Blood pressure
Sleep data (wearables)
Red Flag Values – Seek Medical Attention:
Hematocrit >55%
BP >160/100
Chest pain, breathlessness, vision changes
Final Note: TRT is most effective when paired with proper lifestyle support: exercise, sleep, nutrition, stress management, and a qualified provider who adjusts your treatment slowly and methodically. Don’t rush the process. Respect your biology.