How to Optimise Your TRT Through Blood Testing
Testosterone replacement therapy (TRT) has helped countless men restore energy, mood, libido, and quality of life. But starting TRT is only half the equation. The difference between a protocol that merely raises testosterone levels and one that genuinely optimises your health comes down to one thing: consistent, strategic blood testing.
Without regular bloodwork, TRT becomes guesswork. With it, you and your clinician can fine-tune dosing, prevent side effects, and ensure your therapy is delivering real results — not just numbers on a page.
Why Blood Testing Is Non-Negotiable on TRT
Testosterone interacts with dozens of other hormones and metabolic pathways. When you introduce exogenous testosterone, it does not simply raise your testosterone level in isolation. It can:
- Convert to estradiol (E2) via the aromatase enzyme — too much causes water retention, mood changes, and gynecomastia
- Suppress natural production of LH and FSH, affecting fertility
- Increase red blood cell production, raising hematocrit and blood viscosity
- Alter lipid profiles — potentially lowering HDL ("good") cholesterol
- Affect liver enzyme levels, particularly with oral preparations
Each of these downstream effects needs monitoring. Blood tests are the only objective tool that shows whether your protocol is dialled in or needs adjustment.
Essential Markers to Track on TRT
A comprehensive TRT blood panel should include the following markers, each serving a specific purpose:
Hormones
- Total testosterone — your overall testosterone level; aim for the upper-normal range (typically 20-30 nmol/L in Australian labs)
- Free testosterone — the biologically active fraction; often more clinically relevant than total T
- Estradiol (E2, sensitive assay) — monitor aromatisation; elevated E2 causes bloating, mood swings, and nipple sensitivity
- Sex hormone binding globulin (SHBG) — determines how much testosterone is bioavailable; high SHBG means less free T
- Dihydrotestosterone (DHT) — a potent androgen linked to hair loss and prostate growth; worth checking periodically
- Prolactin — elevated levels can cause low libido and erectile dysfunction despite adequate testosterone
Blood Health
- Full blood count (FBC) — includes haemoglobin and hematocrit
- Hematocrit — the percentage of red blood cells in your blood; TRT increases erythropoiesis. Levels above 52-54% warrant intervention
Metabolic and Organ Function
- Lipid panel — total cholesterol, LDL, HDL, triglycerides; TRT can suppress HDL
- Liver enzymes (ALT, AST) — monitor for hepatic stress, especially if combining TRT with other medications
- Fasting glucose and HbA1c — testosterone affects insulin sensitivity; track metabolic health over time
- PSA (prostate-specific antigen) — baseline and annual screening; TRT does not cause prostate cancer but can stimulate existing tissue growth
When to Test: Timing Your Bloodwork
Timing matters enormously for TRT blood tests. Inconsistent timing produces inconsistent data that makes optimisation impossible.
Best Practice for Injectable TRT (Cypionate/Enanthate)
- Test at trough — draw blood immediately before your next injection. This shows your lowest testosterone level and ensures you are not underdosed at any point in your cycle.
- Morning draws preferred — even on TRT, morning blood draws provide the most consistent baseline for comparison
- Fasting for 8-12 hours — required for accurate lipid and glucose readings
Testing Timeline
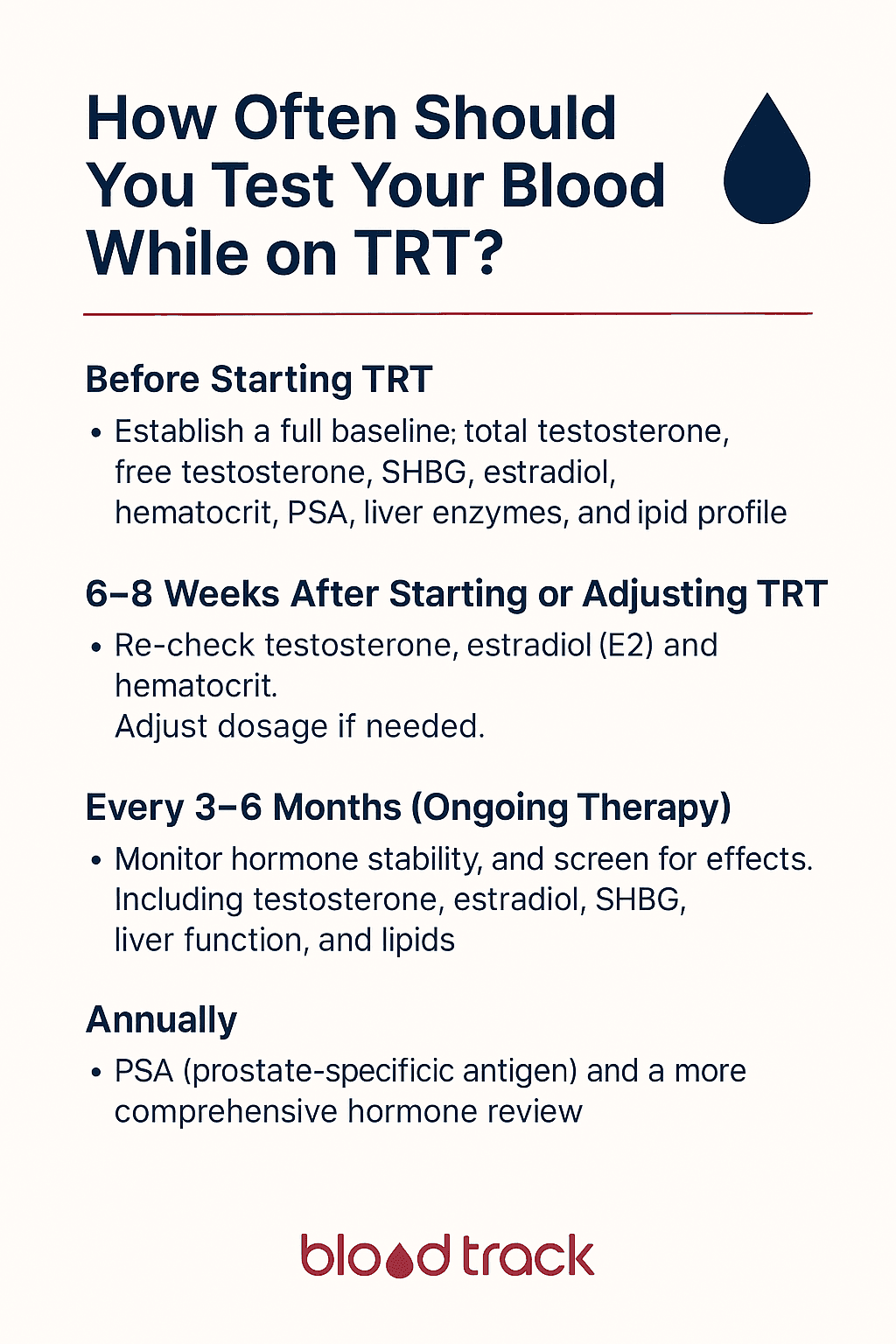
- Before starting TRT: Full baseline panel including total T, free T, E2, SHBG, LH, FSH, prolactin, FBC, lipids, liver function, PSA, thyroid (TSH)
- 6-8 weeks after starting or changing dose: Testosterone, free T, E2, hematocrit. This is the minimum time for levels to stabilise on a new protocol
- Every 3-6 months (stable protocol): Comprehensive panel to monitor ongoing safety and efficacy
- Annually: PSA, full metabolic panel, and comprehensive hormone review
How to Read Your Results for Optimisation
Getting blood drawn is only the first step. Understanding what the numbers mean — and what to do about them — is where optimisation happens.
Testosterone Levels
Most men feel best with trough total testosterone in the upper-normal range (25-35 nmol/L) and free testosterone in the upper quartile of the reference range. If your trough level is below 15 nmol/L, your dose may need increasing. If it is supraphysiological (above 40 nmol/L at trough), you may be overdosing.
Estradiol Management
Estradiol is often the most challenging marker to manage on TRT. Symptoms of high E2 include water retention, emotional sensitivity, and breast tenderness. Symptoms of low E2 include joint pain, low libido, and dry skin. The goal is not to eliminate E2 — it is cardioprotective and essential for bone health — but to keep it proportional to your testosterone level.
Hematocrit Monitoring
Hematocrit above 52-54% increases blood viscosity and cardiovascular risk. If your hematocrit is trending upward, strategies include increasing injection frequency (smaller, more frequent doses reduce peaks), staying well hydrated, donating blood, or reducing your dose.
Common Optimisation Mistakes
- Testing at peak instead of trough — peak values look impressive but do not reflect your lowest point, masking potential underdosing
- Changing dose too frequently — allow 6-8 weeks minimum between adjustments for levels to stabilise
- Ignoring estradiol — many men focus only on testosterone and miss E2-related side effects
- Not tracking trends — a single test tells you very little; trending multiple results reveals whether your protocol is stable, improving, or deteriorating
- Skipping baseline labs — without pre-TRT values, you have no reference point for what is "normal" for your body
Using BloodTrack for TRT Optimisation
BloodTrack was designed with TRT users as a primary audience. Upload your pathology reports and the app automatically extracts testosterone, estradiol, SHBG, hematocrit, and all other relevant markers. Visualise trends across multiple tests, compare results from different protocol phases, and export clean summaries for your clinician.
When you can see your hormone data plotted over months of treatment — with dose changes annotated alongside — optimisation becomes straightforward rather than speculative.
This article is for informational purposes only and does not constitute medical advice. Always consult your GP or healthcare provider for personalised guidance on TRT.